Changing Patient Population
My current job is as clinical faculty at a dental school – I oversee mostly third and fourth year dental students as they learn to diagnose, treatment plan, and practice a variety of procedures on adult patients. The kinds of patients that these students see are quite complex with regards to medical history, oral health needs, and limited finances. Though we always teach to create an ideal treatment plan, patients often are unable to afford even the decreased fees. A lot of patients admit to neglecting their teeth due to kids, work, family issues, lack of time, lack of finances, lack of dental knowledge, or they only utilize emergency care by choice on an as needed basis. The preventive aspect of dental and oral health is something that is often neglected, ignored, or is not that important within the scope of peoples’ lives and they often end up at an institution like ours as a result.
An increasing number of patients are coming to the dental school wanting a second opinion. There is a general mistrust of dentists and their motives with regard to treatment planning and I do not think these feelings are unfounded. We have had a number of patients who come to the dental school with treatment plan in hand for multiple crowns, fillings, bone grafts, implants, etc. that are unnecessary according to what is currently taught in dental schools. In my opinion, we are now in the era of the business model that places more of an interest on newer, faster, and production based dentistry rather than a value and quality-driven education based understanding of one’s health.
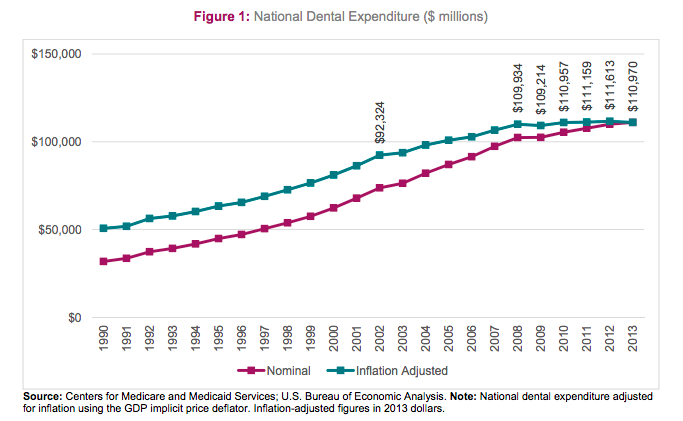
The utilization of dental care has declined among adults aged 20-40, particularly in the young and poor populations. According to this ADA study, this decline in utilization is unrelated to the recent economic downturn. Dental benefits coverage for adults has steadily declined for this population over the past ten years. Conversely, dental care utilization among children has increased steadily over the last ten years due to the expansion of public programs. The Affordable Care Act will expand benefits for dental coverage for children but does not address the population showing the greatest decline in utilization of dental care. Dental benefits are a major predictor of dental utilization among adults, meaning that the lack of expansion for low-income adults and young adults may have long-term consequences to our populations overall oral health.The decline in utilization has not been offset by an increase in per-patient expenditures according to a study by the ADA and Health Policy Institute. In order to make up for a decline in utilization, expenses for existing patients would have to increase significantly to make up for this loss. However, since 2008 per-patient expenditures have been flat. The highest per patient dental expenditures of any group is senior citizens. According to the Health Policy Institute study, Americans ages 60-79 will account for 32% of all dental expenditures by 2040 followed by children at 24%. 
The growth in diversity of our population will likely have an effect on dental utilization trends as well. Racial and ethnic minorities are less likely to utilize dental care than whites according to numerous studies including this one. The Census Bureau projects the Hispanic immigrant population to grow by 57% from 2015 to 2050. Hispanics are less likely than the general population to seek and receive healthcare though they are more likely to experience oral health problems. Knowledge gaps, cost, and language or cultural differences are the top barriers to Hispanics seeking regular dental care according to a study published in 2011.
Changing Attitudes and Philosophy of Care
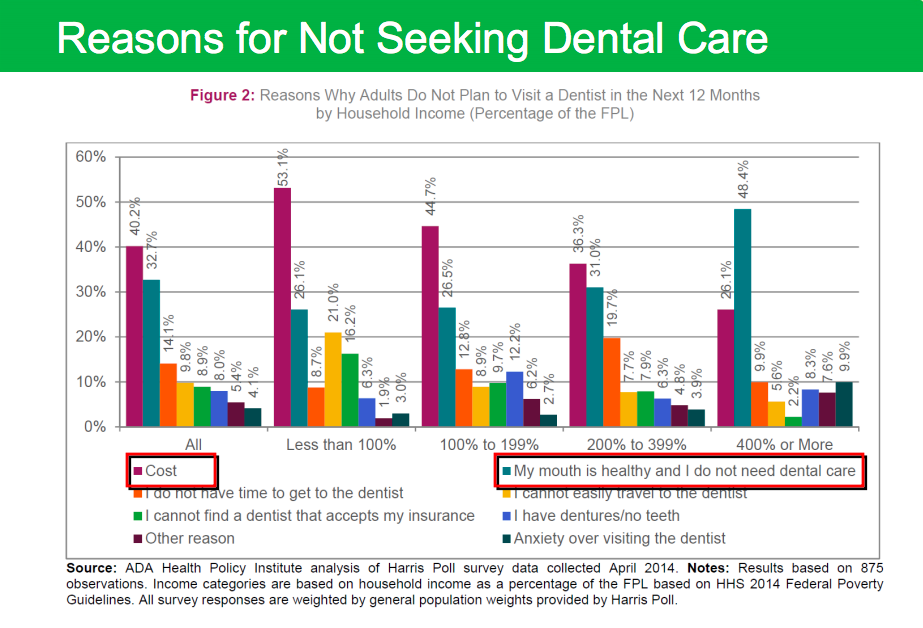
Consumers are changing the way they access care and have become active participants in making decisions regarding their health. Compared to health care, most young adults pay out-of-pocket for dental care which encourages them to compare prices and shop around for value and quality. Since dental care-seeking behavior is strongly associated with having dental benefits, a lot of 20-somethings end up delaying dental care. The ADA states that:
‘More than three-quarters of individuals without dental benefits report having gone to the dentist only once or not at all in the last 10 years. Individuals who lack dental coverage are three times as likely to go to the dentist only when they have a problem rather than for preventive care. Financial barriers and not knowing how much treatments cost are the two most common reasons for delaying dental care.’ (Link to Full Article)
As the population shifts and becomes more diverse we can see changing attitudes towards dentistry. About half of Hispanics do not feel dental visits are necessary as long as they have good home care. However study after study continue to show that the prevalence of disease is higher in minority populations. A new study from the Centers for Disease Control and Prevention (CDC) confirms that nearly one out of two U.S. adults age 30 and over—64.7 million Americans—has periodontitis, the advanced form of periodontal disease. “Periodontitis prevalence was highest in Hispanics (63.5%) and non-Hispanic blacks (59.1%), followed by non-Hispanic Asian Americans (50.0%), and lowest in non-Hispanic whites (40.8%). Prevalence varied two-fold between the lowest and highest levels of socioeconomic status, whether defined by poverty or education.” (Journal of Periodontology Article)
The other attitude change is within the industry itself. After doing some research into what some dental supply companies are forecasting for the future of dentistry, I came across a presentation given to Straumann representatives by their chairman (Mr. Gilbert Achermann) in 2012. The thing that struck me was the statement that ‘economic pressure in developed countries fosters ‘good-enough’ mentality among patients and dentists’. It is sad to see that due to the economic climate, even implant companies are noting the change from quality driven patient-centered dentistry to a more production driven practice model with a decreased standard of care.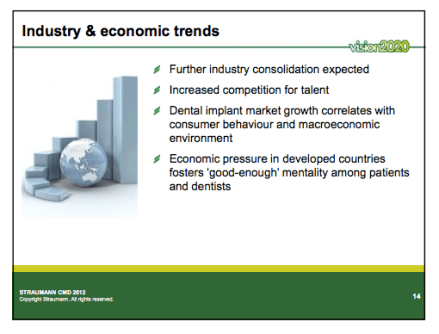
The ADA states that ‘The trend towards larger, consolidated multi-site practices will continue, driven by changes in practice patters of new dentists, a drive for efficiency, and increased competition for patients.’ Is this what is best for our patients? For us? Here is another slide from the presentation by Mr. Achermann of Straumann:
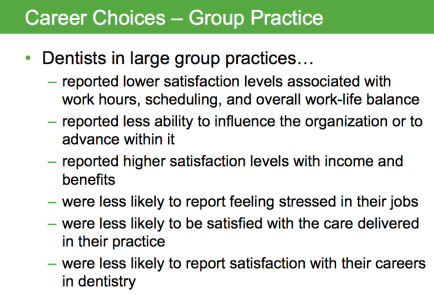
The care delivery model is changing but it is unclear what the most common practice type will be in the future.
Debt
Student debt, the cost of earning a degree, has become outlandish. According to the American Dental Education Association website, only 20% of dental school graduates from the class of 2014 reported <$100,000 debt. Average debt for public dental school graduates was $216,437 and for private dental school graduates it was $289,897. The scariest number I saw was that over 30% of indebted dental school graduates in the class of 2014 reported debt greater than $300,000. The current interest rates on Stafford (6.8%) and Grad PLUS Loans (7.21%) inflate those initial numbers significantly. In order to pay off loans (average of private/public school debt -$253,167) at 7% interest in 10 years, you have to make ~$3000 payments each month with a total interest paid of just shy of $100,000. Who wouldn’t feel the pressure to have to produce?
The ADEA website says in its “Good News” section of the educational debt website, “Dental school graduates have a great reputation for timely repayment.” This is a skewed statement because as of ten years ago, dentists could refinance their loans at a lower rate (some practicing dentists reported rates at 3% or lower) relatively easily. Dental student debt has doubled since 2001 – I’m not sure that my generation of dentists will have the same repayment capabilities as past generations especially if they need to provide for their families, savings, and retirement.
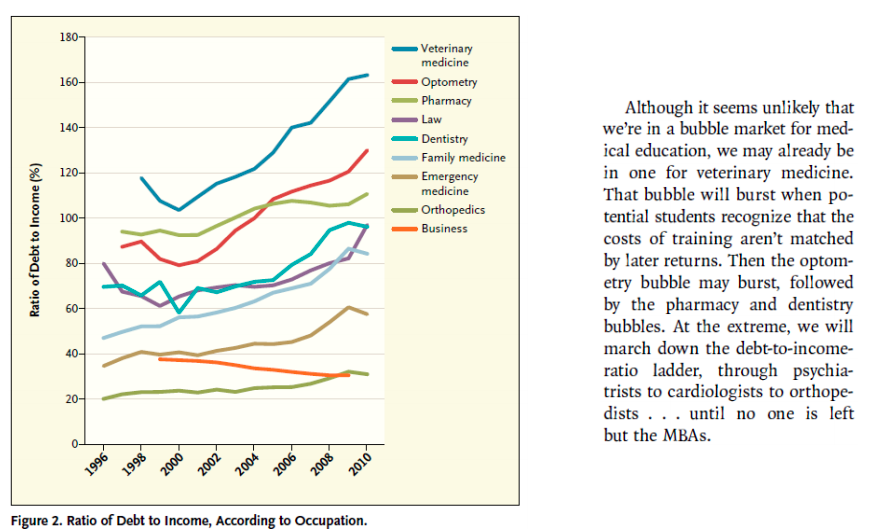
The most astounding figures that I saw were in a study done by the American Dental Association regarding debt to income ratios. A debt income ratio is the percentage of a person’s monthly gross income that goes towards paying debts.

Of course new graduates feel the burden of debt and will feel compelled to seek employment based on income. Most dental students that I teach intend to own their own dental practice but the evolution of the multi-site practice has been relatively new. Also, the mounting debt accumulated during their training may make it more difficult for dentists to purchase practices.
After completing a general practice residency, I sought employment as a general dentist and noticed that most offices wanted to bring on an associate who could do everything: implants, braces, sedation, oral surgery, fillings, crowns, dentures, root canals, etc. The reason was primarily to keep more dentistry in the office to increase production and secondarily for patient convenience (not having to go to another office for treatment). However my concern was always that this was not in the best interest of the patient’s overall oral health. I know a few dentists who are gifted and can do nearly all dental procedures with extreme precision and masterful results. However, they are the exception rather than the rule. In my opinion, recognizing your limitations is an important part of any career. Although going to see a specialist may be inconvenient or more expensive, I refer my patients to specialists because I want my patient to have the best possible long-term outcome. Their health and well-being are more important to me than losing out on potential income. To me, ‘good enough’ isn’t enough.
Supply and Demand of Dentists
The demand for dental care has slowed in recent years and appears to have stabilized at a ‘new normal’. However, the supplyof dentists has continued to increase in part due to a perceived shortage of dentists but also, according to the ADA, the ‘presence of a significant excess demand for dental education.’ The economic collapse also prevented older dentists from retiring which meant that the demand for dentists may increase as the retirement age normalizes. The average age of retirement for dentists was 68.3 in 2011 and has since increased. Given the sluggish dental economy and decreased utilization of care in the young working population, the increase in dental school enrollment could potentially have negative effects on dentists earnings. 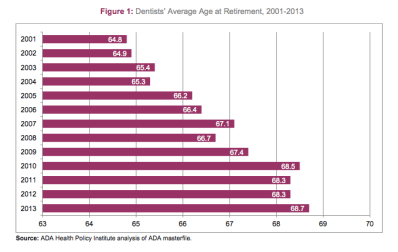
Insurance
One of the largest challenges in dentistry is dental insurance. Dental insurance first started in the mid-1960s and Delta Dental offered insurance with a $1,000 yearly limit in 1972. Many plans today in 2015 have the same $1,000 cap. As you can imagine, 40 years ago $1000 covered a lot of dental procedures. To put it in perspective a gold crown cost approximately $100 in 1970 and today a gold crown costs approximately $1200+. Employers offering dental insurance continue to place pressure on the insurance companies to reduce costs and often default to reducing coverage to keep premium levels consistent. As a result, benefits and spending decrease for the employee. Dental insurance is more of a discount plan rather than ‘insurance’. With standard health insurance you are responsible for your deductible payment and then a significantly smaller portion of the remaining bill. Dental benefits are the opposite, you receive a specific amount of coverage (approx. $1000/year for many, equivalent to 1 crown) and then you are responsible for the entire remaining balance of your bill. Once you reach your yearly maximum, you can wait until the following year for more work or pay out of pocket. For most healthy people, dental insurance is unnecessary. If your dental needs include standard cleanings, exams and x-rays you will lose money by having dental insurance. Premiums are generally $50/month which equates to $600/year. While these preventive services would be completely covered by insurance, if you paid out of pocket you would probably spend around $400/year instead of $600/year on your premium. If dental coverage is provided by your employer, it does make sense to utilize it especially if you can get the whole family’s preventive care covered.
One issue I ran into in private practice is what is called the ‘waiting’ or ‘probationary’ period. A patient would come in and say that they just got dental insurance through work and they are ready to start treatment. However, their plan would have a waiting period of one year for major work (crowns, root canals, oral surgery, etc) and a waiting period of 6 months for minor work (fillings). Insurance companies understand that if you need a filling or a crown, you shouldn’t wait a long time to get them done. If you wait, you risk the situation getting worse, risk having discomfort, or in the worst case scenario – losing your tooth. Unfortunately, even if you need a tooth extracted it wouldn’t be covered until the 1 year probationary period passed.
Conclusion
Ultimately the best dental insurance is prevention – brushing and flossing regularly, getting professional cleanings every six months, and going to a dentist who does high quality work that lasts for years. Rather than searching for the best deal online, it is worth finding a dentist whom you trust and with whom you can build a relationship. Having a consistent history of your dental health helps dental professionals make clinical decisions regarding your teeth and we are less likely to redo our own work and more likely to redo someone elses based on x-rays and limited information. The trends in dental care utilization, population demographics, consumerism, educational costs, and legislation have changed the landscape of dentistry significantly. I hope that we are all ready for the changes and can hold on to what we feel is important for the future of our profession.

{kind=link}